How To Prevent Heel Spur

Overview
Heel spurs are a bone growth that extends from the heel bone, particularly on the bottom front of the heel bone and sometimes slightly to the side. Usually, a heel spur forms where the plantar fascia ligament attaches to the bottom of the heel bone. Those who overuse, or put heavy stress on the plantar fascia, are at risk of developing heel spurs.
Causes
Heel spurs form in some patients who have plantar fasciitis (PLAN-tar fash-ee-I-tis), and tend to occur in patients who have had the problem for a prolonged period of time. While about 70 percent of patients with plantar fasciitis have a heel spur, X-rays also show about 50 percent of patients with no symptoms of plantar fasciitis also have a heel spur.

Symptoms
Pain and discomfort associated with heel spurs does not occur from the spur itself. The bone growth itself has no feeling. However, as you move, this growth digs into sensitive nerves and tissue along the heel of the foot, resulting in severe pain. Pain can also be generated when pushing off with the toes while walking. Swelling along the heel is also common.
Diagnosis
A Heel Spur diagnosis is made when an X-ray shows a hook of bone protruding from the bottom of the foot at the point where the plantar fascia is attached to the heel bone. The plantar fascia is the thick, connective tissue that runs from the calcaneus (heel bone) to the ball of the foot. This strong and tight tissue helps maintain the arch of the foot. It is also one of the major transmitters of weight across the foot as you walk or run. In other words, tremendous stress is placed on the plantar fascia.
Non Surgical Treatment
If pain and other symptoms of inflammation-redness, swelling, heat-persist, you should limit normal daily activities and contact a doctor of podiatric medicine. The podiatric physician will examine the area and may perform diagnostic X-rays to rule out problems of the bone. Early treatment might involve oral or injectable anti-inflammatory medication, exercise and shoe recommendations, taping or strapping, or use of shoe inserts or orthotic devices. Taping or strapping supports the foot, placing stressed muscles and tendons in a physiologically restful state. Physical therapy may be used in conjunction with such treatments. A functional orthotic device may be prescribed for correcting biomechanical imbalance, controlling excessive pronation, and supporting of the ligaments and tendons attaching to the heel bone. It will effectively treat the majority of heel and arch pain without the need for surgery. Only a relatively few cases of heel pain require more advanced treatments or surgery. If surgery is necessary, it may involve the release of the plantar fascia, removal of a spur, removal of a bursa, or removal of a neuroma or other soft-tissue growth.
Surgical Treatment
More than 90 percent of people get better with nonsurgical treatments. If conservative treatment fails to treat symptoms of heel spurs after a period of 9 to 12 months, surgery may be necessary to relieve pain and restore mobility. Surgical techniques include release of the plantar fascia, removal of a spur. Pre-surgical tests or exams are required to identify optimal candidates, and it's important to observe post-surgical recommendations concerning rest, ice, compression, elevation of the foot, and when to place weight on the operated foot. In some cases, it may be necessary for patients to use bandages, splints, casts, surgical shoes, crutches, or canes after surgery. Possible complications of heel surgery include nerve pain, recurrent heel pain, permanent numbness of the area, infection, and scarring. In addition, with plantar fascia release, there is risk of instability, foot cramps, stress fracture, and tendinitis.
What Is Bursitis In The Foot?
Overview
Retrocalcaneal bursitis is the inflammation of the retrocalcaneal bursa, which is located behind the heel bone, also known as the calcaneal bone (hence the name retrocalcaneal). The retrocalcaneal bursa is a thin, slippery, fluid-filled sac that serves as a both a cushion and lubricant between the heel bone and the Achilles tendon. Inflammation of the retrocalcaneal bursa usually results from irritation of the bursa. This irritation may be due to certain activities, an underlying health condition such as arthritis, or an abnormality of the foot, such the development of a boney prominence on the calcaneal bone, called a Haglund's deformity.
Causes
Retrocalcaneal bursitis can be caused through injury or infection or be can be triggered by certain health conditions. If bursitis develops as a result of injury then it will normally be due to a repetitive strenuous activity that encourages the calf muscles (the gastrocnemius and soleus muscle), which attach to the heel bone via the Achilles tendon, to tighten and shorten from overuse, for example repetitively wearing high heels, running and even wearing tight shoes that pinch at the back of the heel. This puts more pressure over the bursa as the tendon rubs more tightly over it, irritating it and triggering a painful inflammatory reaction (swelling). This risk of developing bursitis in this way is greater for those whose jobs or hobbies involve a lot of repetitive movements, for example carpet fitters and gardeners who spend a lot of time kneeling and so are more at risk of bursitis in the knee. Runners have a greater likelihood of developing bursitis in the hip. Bursitis can also be brought on by excessive pressure or direct impact trauma, such as banging your elbow or dropping on to your knees. Infection is a less common cause of bursitis and normally only occurs in people who have a weakened immune system from other health issues. The infection can work its way to the bursa from a cut close to the bursa that has become infected, in these cases the bursitis is termed as septic bursitis. Certain health conditions can also trigger the development of bursitis, such as rheumatoid arthritis and gout, amongst others.
Symptoms
The main symptom of heel bursitis is pain. You may experience pain in your heel when you walk or run. There may also be pain if the area is touched or if you stand on your tiptoes. In addition to pain, the area may appear red and warm, which are both signs of inflammation. Even if you have these symptoms, only a doctor can determine if you have bursitis of the heel. Your doctor will use these symptoms along with a general exam to determine if you are suffering from bursitis of the heel.
Diagnosis
The diagnosis is based on the symptoms and an examination. For anterior Achilles tendon bursitis, doctors use x-rays to rule out a fracture of the heel bone or damage to the heel bone caused by rheumatoid arthritis or other inflammatory arthritis.
Non Surgical Treatment
The patient with retrocalcaneal bursitis should be instructed to apply ice to the posterior heel and ankle in the acute period of the bursitis. Icing can be performed several times a day, for 15-20 minutes each. Some clinicians also advocate the use of contrast baths. Gradual progressive stretching of the Achilles tendon may help relieve impingement on the subtendinous bursa and can be performed in the following manner. Stand in front of a wall, with the affected foot flat on the floor. Lean forward toward the wall until a gentle stretching is felt within the ipsilateral Achilles tendon. Maintain the stretch for 20-60 seconds and then relax. Perform the stretches with the knee extended and then again with the knee flexed. To maximize the benefit of the stretching program, repeat the above steps for several stretches per set, several times daily. Avoid ballistic (ie, abrupt, jerking) stretches. Other treatment options are microcurrent therapy and corticosteriod injection into the retrocalcaneal bursa. If conservation treatment fails then surgery is indicated.
Surgical Treatment
Surgery. Though rare, particularly challenging cases of retrocalcaneal bursitis might warrant a bursectomy, in which the troublesome bursa is removed from the back of the ankle. Surgery can be effective, but operating on this boney area can cause complications, such as trouble with skin healing at the incision site. In addition to removing the bursa, a doctor may use the surgery to treat another condition associated with the retrocalcaneal bursitis. For example, a surgeon may remove a sliver of bone from the back of the heel to alter foot mechanics and reduce future friction. Any bone spurs located where the Achilles attaches to the heel may also be removed. Regardless of the conservative treatment that is provided, it is important to wait until all pain and swelling around the back of the heel is gone before resuming activities. This may take several weeks. Once symptoms are gone, a patient may make a gradual return to his or her activity level before their bursitis symptoms began. Returning to activities that cause friction or stress on the bursa before it is healed will likely cause bursitis symptoms to flare up again.
Retrocalcaneal bursitis is the inflammation of the retrocalcaneal bursa, which is located behind the heel bone, also known as the calcaneal bone (hence the name retrocalcaneal). The retrocalcaneal bursa is a thin, slippery, fluid-filled sac that serves as a both a cushion and lubricant between the heel bone and the Achilles tendon. Inflammation of the retrocalcaneal bursa usually results from irritation of the bursa. This irritation may be due to certain activities, an underlying health condition such as arthritis, or an abnormality of the foot, such the development of a boney prominence on the calcaneal bone, called a Haglund's deformity.
Causes
Retrocalcaneal bursitis can be caused through injury or infection or be can be triggered by certain health conditions. If bursitis develops as a result of injury then it will normally be due to a repetitive strenuous activity that encourages the calf muscles (the gastrocnemius and soleus muscle), which attach to the heel bone via the Achilles tendon, to tighten and shorten from overuse, for example repetitively wearing high heels, running and even wearing tight shoes that pinch at the back of the heel. This puts more pressure over the bursa as the tendon rubs more tightly over it, irritating it and triggering a painful inflammatory reaction (swelling). This risk of developing bursitis in this way is greater for those whose jobs or hobbies involve a lot of repetitive movements, for example carpet fitters and gardeners who spend a lot of time kneeling and so are more at risk of bursitis in the knee. Runners have a greater likelihood of developing bursitis in the hip. Bursitis can also be brought on by excessive pressure or direct impact trauma, such as banging your elbow or dropping on to your knees. Infection is a less common cause of bursitis and normally only occurs in people who have a weakened immune system from other health issues. The infection can work its way to the bursa from a cut close to the bursa that has become infected, in these cases the bursitis is termed as septic bursitis. Certain health conditions can also trigger the development of bursitis, such as rheumatoid arthritis and gout, amongst others.
Symptoms
The main symptom of heel bursitis is pain. You may experience pain in your heel when you walk or run. There may also be pain if the area is touched or if you stand on your tiptoes. In addition to pain, the area may appear red and warm, which are both signs of inflammation. Even if you have these symptoms, only a doctor can determine if you have bursitis of the heel. Your doctor will use these symptoms along with a general exam to determine if you are suffering from bursitis of the heel.
Diagnosis
The diagnosis is based on the symptoms and an examination. For anterior Achilles tendon bursitis, doctors use x-rays to rule out a fracture of the heel bone or damage to the heel bone caused by rheumatoid arthritis or other inflammatory arthritis.
Non Surgical Treatment
The patient with retrocalcaneal bursitis should be instructed to apply ice to the posterior heel and ankle in the acute period of the bursitis. Icing can be performed several times a day, for 15-20 minutes each. Some clinicians also advocate the use of contrast baths. Gradual progressive stretching of the Achilles tendon may help relieve impingement on the subtendinous bursa and can be performed in the following manner. Stand in front of a wall, with the affected foot flat on the floor. Lean forward toward the wall until a gentle stretching is felt within the ipsilateral Achilles tendon. Maintain the stretch for 20-60 seconds and then relax. Perform the stretches with the knee extended and then again with the knee flexed. To maximize the benefit of the stretching program, repeat the above steps for several stretches per set, several times daily. Avoid ballistic (ie, abrupt, jerking) stretches. Other treatment options are microcurrent therapy and corticosteriod injection into the retrocalcaneal bursa. If conservation treatment fails then surgery is indicated.
Surgical Treatment
Surgery. Though rare, particularly challenging cases of retrocalcaneal bursitis might warrant a bursectomy, in which the troublesome bursa is removed from the back of the ankle. Surgery can be effective, but operating on this boney area can cause complications, such as trouble with skin healing at the incision site. In addition to removing the bursa, a doctor may use the surgery to treat another condition associated with the retrocalcaneal bursitis. For example, a surgeon may remove a sliver of bone from the back of the heel to alter foot mechanics and reduce future friction. Any bone spurs located where the Achilles attaches to the heel may also be removed. Regardless of the conservative treatment that is provided, it is important to wait until all pain and swelling around the back of the heel is gone before resuming activities. This may take several weeks. Once symptoms are gone, a patient may make a gradual return to his or her activity level before their bursitis symptoms began. Returning to activities that cause friction or stress on the bursa before it is healed will likely cause bursitis symptoms to flare up again.
Recovery After Bunion Hammer Toe Surgery
 Overview
Overview
hammertoe can affect any of the toes on the foot except the big toe, though the most common toe to suffer is the second one. While the smallest toe can be affected, the condition causes the toe to twist out to the side rather than to curl forward. Hammertoe is not very discriminating; it may appear on all four toes of the foot or on only one toe, depending on the cause.
Causes
Your toe hammertoes contains two joints that allow it to bend at the middle and bottom. A hammertoe occurs when the middle joint becomes dislocated. Common causes of this joint dislocation include a toe injury, arthritis, a high foot arch, wearing shoes that don?t fit properly, tightened ligaments or tendons in the foot, pressure from a bunion (when your big toe points inward toward your second toe) Spinal cord or peripheral nerve damage may cause all of your toes to curl downward.
 Symptoms
Symptoms
A hammer toe may be painful, especially when irritated by a shoe. All four toe conditions may cause cramps in the toes, foot and leg due to the abnormal function of the tendons in the foot. If a mallet toe has occurred, you are likely to suffer from a corn at the end of the toe. A hammertoe may cause a corn on the top of the toe. Infections and ulcers can also occur. In severe cases a mallet toe, trigger toe, claw toe or a hammer toe may create a downward pressure on the foot, which can result in hard skin and corns on the soles of the feet.
Diagnosis
Your healthcare provider will examine your foot, checking for redness, swelling, corns, and calluses. Your provider will also measure the flexibility of your toes and test how much feeling you have in your toes. You may have blood tests to check for arthritis, diabetes, and infection.
Non Surgical Treatment
Your podiatrist may recommend conservative treatment techniques for your hammertoes based on your foot structure, which will likely involve removing any thick, painful skin, padding your painful area, and recommending for you shoes that give your curled toes adequate room. Conservative care strategies for this health purpose may also involve the use of Correct Toes, our toe straightening and toe spacing device.
Surgical Treatment
Hammer toe can be corrected by surgery if conservative measures fail. Usually, surgery is done on an outpatient basis with a local anesthetic. The actual procedure will depend on the type and extent of the deformity. After the surgery, there may be some stiffness, swelling and redness and the toe may be slightly longer or shorter than before. You will be able to walk, but should not plan any long hikes while the toe heals, and should keep your foot elevated as much as possible.
 Prevention
Prevention
Although these following preventative tips may be able to reverse a painful bunion or hammertoe deformity, they are more effective when applied to young people, and are less effective the longer a person has progressed with their bunion or hammertoe deformity. This is because the joints in our bodies get used to the positions they are most frequently held in, and our feet are no different, with our 12 to 15 hours a day in restrictive footwear, with tapering toeboxes, heel elevation, and toespring.
Overpronation Of The Foot
Overview
Over-pronation is very common and affects millions of Australians. To better understand this condition, we'll take a closer look at the 3 most common foot types. An estimated 70% of the population has fallen arches (or a low arch). Only 20% have a normal arch. And 10% have abnormal feet, in other words they either have flat feet or the opposite, a high arched foot. Most of us have a low arch. The foot actually appears quite normal and a clear (but low) arch is present under the foot, especially when sitting down. The situation changes with weight-bearing: when we get up the arch lowers. When we start walking the arches collapse and the ankles roll inwards. This is called over-pronation or fallen arches. Over-pronation is not the same as flat feet as often noted.
Causes
Over-pronation is very prominent in people who have flexible, flat feet. The framework of the foot begins to collapse, causing the foot to flatten and adding stress to other parts of the foot. As a result, over-pronation, often leads to Plantar Fasciitis, Heel Spurs, Metatarsalgia, Post-tib Tendonitis and/or Bunions. There are many causes of flat feet. Obesity, pregnancy or repetitive pounding on a hard surface can weaken the arch leading to over-pronation. Often people with flat feet do not experience discomfort immediately, and some never suffer from any discomfort at all. However, when symptoms develop and become painful, walking becomes awkward and causes increased strain on the feet and calves.
Symptoms
Overpronation can lead to injuries and pain in the foot, ankle, knee, or hip. Overpronation puts extra stress on all the bones in the feet. The repeated stress on the knees, shins, thighs, and pelvis puts additional stress on the muscles, tendons, and ligaments of the lower leg. This can put the knee, hip, and back out of alignment, and it can become very painful.
Diagnosis
Your healthcare provider will ask about your symptoms, medical history, and activities and examine your feet. Your provider may watch you walk or run. Check the motion of your feet when they strike the ground. Look at your athletic shoes to see if they show an abnormal pattern of wear.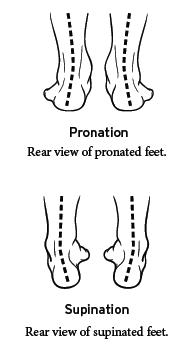
Non Surgical Treatment
Over-Pronation can be treated conservatively (non-surgical treatments) with over-the-counter orthotics. These orthotics should be designed with appropriate arch support and medial rearfoot posting to prevent the over-pronation. Footwear should also be examined to ensure there is a proper fit. Footwear with a firm heel counter is often recommended for extra support and stability. Improper fitting footwear can lead to additional problems of the foot.
Prevention
Custom-made orthotics will reduce the twisting of the leg muscles as they enter the foot, by maintaining a normal alignment of the bones and joints of the foot. If the bones and joints are aligned properly, by reducing the pronation, the muscles can run straight to their attachments in the foot, without twisting to get to these bones. This action of custom-made orthotics will reduce Achilles Tendonitis shin splints; ankle, knee, hip, and lower back pain; and leg cramps. This action will also allow the leg muscles to work more efficiently, thus allowing you to walk and run with less effort.
Over-pronation is very common and affects millions of Australians. To better understand this condition, we'll take a closer look at the 3 most common foot types. An estimated 70% of the population has fallen arches (or a low arch). Only 20% have a normal arch. And 10% have abnormal feet, in other words they either have flat feet or the opposite, a high arched foot. Most of us have a low arch. The foot actually appears quite normal and a clear (but low) arch is present under the foot, especially when sitting down. The situation changes with weight-bearing: when we get up the arch lowers. When we start walking the arches collapse and the ankles roll inwards. This is called over-pronation or fallen arches. Over-pronation is not the same as flat feet as often noted.
Causes
Over-pronation is very prominent in people who have flexible, flat feet. The framework of the foot begins to collapse, causing the foot to flatten and adding stress to other parts of the foot. As a result, over-pronation, often leads to Plantar Fasciitis, Heel Spurs, Metatarsalgia, Post-tib Tendonitis and/or Bunions. There are many causes of flat feet. Obesity, pregnancy or repetitive pounding on a hard surface can weaken the arch leading to over-pronation. Often people with flat feet do not experience discomfort immediately, and some never suffer from any discomfort at all. However, when symptoms develop and become painful, walking becomes awkward and causes increased strain on the feet and calves.
Symptoms
Overpronation can lead to injuries and pain in the foot, ankle, knee, or hip. Overpronation puts extra stress on all the bones in the feet. The repeated stress on the knees, shins, thighs, and pelvis puts additional stress on the muscles, tendons, and ligaments of the lower leg. This can put the knee, hip, and back out of alignment, and it can become very painful.
Diagnosis
Your healthcare provider will ask about your symptoms, medical history, and activities and examine your feet. Your provider may watch you walk or run. Check the motion of your feet when they strike the ground. Look at your athletic shoes to see if they show an abnormal pattern of wear.
Non Surgical Treatment
Over-Pronation can be treated conservatively (non-surgical treatments) with over-the-counter orthotics. These orthotics should be designed with appropriate arch support and medial rearfoot posting to prevent the over-pronation. Footwear should also be examined to ensure there is a proper fit. Footwear with a firm heel counter is often recommended for extra support and stability. Improper fitting footwear can lead to additional problems of the foot.
Prevention
Custom-made orthotics will reduce the twisting of the leg muscles as they enter the foot, by maintaining a normal alignment of the bones and joints of the foot. If the bones and joints are aligned properly, by reducing the pronation, the muscles can run straight to their attachments in the foot, without twisting to get to these bones. This action of custom-made orthotics will reduce Achilles Tendonitis shin splints; ankle, knee, hip, and lower back pain; and leg cramps. This action will also allow the leg muscles to work more efficiently, thus allowing you to walk and run with less effort.
What Exactly Is Severs Disease?
Overview
Sever?s Disease (calcaneal aphophysitis) is not really a disease, but more a repetitious strain injury. This is the most common cause of kids heel pain seen at Podiatry Care. Active children in football, soccer, basketball, netball and tennis with this type of foot pain complain of pain in the region of the heel bone particularly after exercise. In severe cases, children will complain of pain during exercise as well. It is a frequent cause of heel pain in children, particularly in the very active child. It is most often seen in children between the ages of 8 to 15 years as the growth plate is not fully developed or calcified at this time.
Causes
The cause of Sever's disease is not entirely clear. It is most likely due to overuse or repeated minor trauma that happens in a lot of sporting activities - the cartilage join between the two parts of the bone can not take all the shear stress of the activities. Some children seem to be just more prone to it for an unknown reason - combine this with sport, especially if its on a hard surface and the risk of getting it increases. It can be almost epidemic at the start of some sports seasons, especially winter. At the start of winter, the grounds are often harder, but soften later. Children who are heavier are also at greater risk for developing calcaneal apophysitis.
Symptoms
Athletes with Sever?s disease are typically aged 9 to 13 years and participate in running or jumping sports such as soccer, football, basketball, baseball, and gymnastics. The typical complaint is heel pain that develops slowly and occurs with activity. The pain is usually described like a bruise. There is rarely swelling or visible bruising. The pain is usually worse with running in cleats or shoes that have limited heel lift, cushion, and arch support. The pain usually goes away with rest and rarely occurs with low-impact sports such as bicycling, skating, or swimming.
Diagnosis
To diagnose the cause of the child?s heel pain and rule out other more serious conditions, the foot and ankle surgeon obtains a thorough medical history and asks questions about recent activities. The surgeon will also examine the child?s foot and leg. X-rays are often used to evaluate the condition. Other advanced imaging studies and laboratory tests may also be ordered.
Non Surgical Treatment
Treatment is primarily directed towards reducing the amount of stress to the heel. Often a heel lift, is placed in the shoe to reduce the pull of the Achilles tendon on the apophysis. Gel or cushioned heel cups may also be helpful in reducing micro trauma to the heel. Orthotic control may also be indicated when a pathologic condition exists in the foot that may be contributing to the increased heel stress. Occasionally, it becomes necessary for adequate healing, to rest the area completely. This can be accomplished either by complete elimination of all strenuous activities, or by using a walking cast or crutches. Often simply reducing activity levels is adequate. Your physician will discuss the best treatment plan with you and your child.
Prevention
Once your child?s growth spurt ends, and she's reached full size, her Sever?s disease won?t return. Until then, the condition can happen again if your child stays very active. Some simple steps can help prevent it. Have your child. Wear supportive, shock-absorbing shoes. Stretch her calves, heels, and hamstrings. Not overdo it. Warn against over-training, and suggest plenty of rest, especially if she begins to feel pain in her heel. Try to avoid lots of running and pounding on hard surfaces. If she?s overweight, help her lose those extra pounds, which can increase pressure on her heels.
Sever?s Disease (calcaneal aphophysitis) is not really a disease, but more a repetitious strain injury. This is the most common cause of kids heel pain seen at Podiatry Care. Active children in football, soccer, basketball, netball and tennis with this type of foot pain complain of pain in the region of the heel bone particularly after exercise. In severe cases, children will complain of pain during exercise as well. It is a frequent cause of heel pain in children, particularly in the very active child. It is most often seen in children between the ages of 8 to 15 years as the growth plate is not fully developed or calcified at this time.
Causes
The cause of Sever's disease is not entirely clear. It is most likely due to overuse or repeated minor trauma that happens in a lot of sporting activities - the cartilage join between the two parts of the bone can not take all the shear stress of the activities. Some children seem to be just more prone to it for an unknown reason - combine this with sport, especially if its on a hard surface and the risk of getting it increases. It can be almost epidemic at the start of some sports seasons, especially winter. At the start of winter, the grounds are often harder, but soften later. Children who are heavier are also at greater risk for developing calcaneal apophysitis.
Symptoms
Athletes with Sever?s disease are typically aged 9 to 13 years and participate in running or jumping sports such as soccer, football, basketball, baseball, and gymnastics. The typical complaint is heel pain that develops slowly and occurs with activity. The pain is usually described like a bruise. There is rarely swelling or visible bruising. The pain is usually worse with running in cleats or shoes that have limited heel lift, cushion, and arch support. The pain usually goes away with rest and rarely occurs with low-impact sports such as bicycling, skating, or swimming.
Diagnosis
To diagnose the cause of the child?s heel pain and rule out other more serious conditions, the foot and ankle surgeon obtains a thorough medical history and asks questions about recent activities. The surgeon will also examine the child?s foot and leg. X-rays are often used to evaluate the condition. Other advanced imaging studies and laboratory tests may also be ordered.
Non Surgical Treatment
Treatment is primarily directed towards reducing the amount of stress to the heel. Often a heel lift, is placed in the shoe to reduce the pull of the Achilles tendon on the apophysis. Gel or cushioned heel cups may also be helpful in reducing micro trauma to the heel. Orthotic control may also be indicated when a pathologic condition exists in the foot that may be contributing to the increased heel stress. Occasionally, it becomes necessary for adequate healing, to rest the area completely. This can be accomplished either by complete elimination of all strenuous activities, or by using a walking cast or crutches. Often simply reducing activity levels is adequate. Your physician will discuss the best treatment plan with you and your child.
Prevention
Once your child?s growth spurt ends, and she's reached full size, her Sever?s disease won?t return. Until then, the condition can happen again if your child stays very active. Some simple steps can help prevent it. Have your child. Wear supportive, shock-absorbing shoes. Stretch her calves, heels, and hamstrings. Not overdo it. Warn against over-training, and suggest plenty of rest, especially if she begins to feel pain in her heel. Try to avoid lots of running and pounding on hard surfaces. If she?s overweight, help her lose those extra pounds, which can increase pressure on her heels.
Rigid Flat Feet In Adults
Overview
Adult-acquired flatfoot or collapsed arch occurs because the large tendon on the inside of the ankle - the posterior tibial tendon - becomes stretched out and no longer supports the foot?s arch. In many cases, the condition worsens and and the tendon thickens, becoming painful, especially during activities. Flatfoot or collapsed arch is also known as posterior tibial tendon dysfunction. This condition is different than having flat feet since birth (known as congenital flatfoot), although sometimes these patients develop similar symptoms and require similar treatments. 
Causes
There are numerous causes of acquired Adult Flatfoot, including, trauma, fracture, dislocation, tendon rupture/partial rupture or inflammation of the tendons, tarsal coalition, arthritis, neuroarthropathy and neurologic weakness. The most common cause of acquired Adult Flatfoot is due to overuse of a tendon on the inside of the ankle called the posterior tibial tendon. This is classed as - posterior tibial tendon dysfunction. What are the causes of Adult Acquired flat foot? Trauma, Fracture or dislocation. Tendon rupture, partial tear or inflammation. Tarsal Coalition. Arthritis. Neuroarthropathy. Neurological weakness.
Symptoms
Symptoms are minor and may go unnoticed, Pain dominates, rather than deformity. Minor swelling may be visible along the course of the tendon. Pain and swelling along the course of the tendon. Visible decrease in arch height. Aduction of the forefoot on rearfoot. Subluxed tali and navicular joints. Deformation at this point is still flexible. Considerable deformity and weakness. Significant pain. Arthritic changes in the tarsal joints. Deformation at this point is rigid.
Diagnosis
The diagnosis of posterior tibial tendon dysfunction and AAFD is usually made from a combination of symptoms, physical exam and x-ray imaging. The location of pain, shape of the foot, flexibility of the hindfoot joints and gait all may help your physician make the diagnosis and also assess how advanced the problem is.
Non surgical Treatment
Nonoperative therapy for posterior tibial tendon dysfunction has been shown to yield 67% good-to-excellent results in 49 patients with stage 2 and 3 deformities. A rigid UCBL orthosis with a medial forefoot post was used in nonobese patients with flexible heel deformities correctible to neutral and less than 10? of forefoot varus. A molded ankle foot orthosis was used in obese patients with fixed deformity and forefoot varus greater than 10?. Average length of orthotic use was 15 months. Four patients ultimately elected to have surgery. The authors concluded that orthotic management is successful in older low-demand patients and that surgical treatment can be reserved for those patients who fail nonoperative treatment. 
Surgical Treatment
For patients with a more severe deformity, or significant symptoms that do not respond to conservative treatment, surgery may be necessary. There are several procedures available depending on the nature of your condition. Ligament and muscle lengthening, removal of inflamed tendon lining, transferring of a nearby tendon to re-establish an arch, and bone realignment and fusion are examples of surgical options to help with a painful flatfoot condition. Surgery can be avoided when symptoms are addressed early. If you are feeling ankle pain or notice any warmth, redness or swelling in your foot, contact us immediately. We can create a tailored treatment plan to resolve your symptoms and prevent future problems.
Heel And Arch Pain Exercises
Overview
A flat foot is a term used to described a collapsed arch. Medically, the term is pes planovalgus (for foot flatten and pushed outwards). There are varying degrees of ?flatness?. Though not all flat feet are problematic, however, when there are painful flat feet can cause significant discomfort and activity limitations. There are two kinds of flat feet - flexible (mobile) or rigid (stiff). A flexible flat foot is one where the foot retains motion, and the arch is able to be recreated when there is no weight on the foot. In contrast, a rigid flat foot is ?stuck? in the flat position regardless of whether or not there is pressure placed on the foot.

Causes
There are a variety of causes of flat feet. Flat feet can be genetic, acquired and develop over time. Young children and teens can have no arches. Injury can lead to flat feet. Tendon problems, and arthritis can lead to flat feet. Rigid flat feet may occur from a condition called tarsal coalition, where the bones in the back of the foot are genetically fused or locked together.
Symptoms
Repetitive exertive activity arch pain is usually sharp, and localized to a specific area, rather than the entire arch. Usually the pain occurs in the area just in front of the heel. It is present when first standing on the foot in the morning, but may decrease once you start walking around, but will, gradually becomes worse with continued walking or running. Swelling may be present. The pain subsides with rest, but stretching the arch while resting may cause the pain to return. Injury pain is constantly present, but worse when standing on the foot. This pain is localized to a specific area, but may radiate out from this area to the entire foot. The pain is sharp, and usually accompanied by swelling and occasionally "black and blue" discolorations. The pain due to the natural aging process is usually dull and aching, or stiff, and can be felt throughout the entire arch area, rather then in just one spot. This pain is present whenever weight bearing, and usually becomes worse with continued walking. The pain gradually subsides when resting, and usually does not return with stretching. Biomechanical defect pain is usually localized to a section of the arch, such as the inner, middle, outer, front, or back of the arch. This pain may be sharp or dull, but is always worse with continued walking.
Diagnosis
The doctor will take a brief history to determine how the injury occurred. If necessary, a thorough physical exam may be conducted to evaluate for any other injuries. Taking your workout shoes to the exam may also provide valuable information to the medical practitioner. Both feet will be physically and visually examined by the medical practitioner. The foot and arch will be touched and manipulated possibly with a lot of pressure and inspected to identify obvious deformities, tender spots, or any differences in the bones of the foot and arch.
Non Surgical Treatment
A new ankle foot orthosis known as the Richie Brace, offered by PAL Health Systems, has proven to show significant success in treating Stage II posterior tibial dysfunction and the adult acquired flatfoot. This is a sport-style brace connected to a custom corrected foot orthotic device that fits well into most forms of lace-up footwear, including athletic shoes. The brace is light weight and far more cosmetically appealing than the traditional ankle foot orthosis previously prescribed.

Surgical Treatment
The procedure involves cutting and shifting the bone, and then performing a tendon transfer. First, the surgeon performs a calcaneal osteotomy, cutting the heel bone and shifting it into the correct position. Second, the surgeon transfers the tendon. Reroute the flexor digitorum to replace the troublesome posterior tibial tendon. Finally, the surgeon typically performs one or more fine-tuning procedures that address the patient?s specific foot deformity. Often, the surgeon will lengthen the Achilles tendon because it is common for the mispositioned foot to cause the Achilles to tighten. Occasionally, to increase the arch, the surgeon performs another osteotomy of one of the bones of the midfoot. Occasionally, to point the foot in a straightforward direction, the surgeon performs another osteotomy of the outside portion of the calcaneus.
Prevention
Early in the treatment of arch pain, consideration needs to be given to the cause and strategies put in place to prevent it happening again. Advice should be sought on the adequacy of footwear. Stretching exercises should be continued long after the symptoms are gone. Foot orthoses should be used if structural imbalances are present. Activity levels and types of activities (occupational and sporting) need to be considered and modified accordingly.
Stretching Exercises
Easy Beginner Version. Start with your bare foot on a flat surface, toes spread out. Place a penny under the ball of your foot and the end of a pen under the middle of your arch (sticking out from the inside of your foot). Activate your arch by flexing your arch muscle. You should feel the muscles on the ball of your foot pushing down on the penny, but your arch shouldn't be pushing down on the pen. These tools help you (1) avoid rolling your foot and (2) avoid pressing down with your toes (as an extra tip, you can slide a business card under your toes before doing the exercise-when you activate your arch, you should be able to slide the business card out easily with your fingers). Do your best to keep your toes relaxed. Advanced Version. Once you're ready to move on, you can try this advanced version. It builds on the above exercise to incorporate full body twisting and balance, helping you to maintain proper arches while you move. Using the same ideas from above, stand on a flat surface in your bare feet with a penny under the ball of your foot and the end of a pen under your arch. This time, stand with your back a few inches away form a wall or a door. Lift your other leg (the one without the penny or pen) and stand on one foot. Use the wall for balance, if necessary. Lift one arm and stretch it across your body until you touch the wall or door on the opposite side, maintaining a straight back. Keep your foot straight and your arch on the penny but above the pen. Your arch will want to follow the movement and roll off, but you will need to activate it to stay stable during the movement. Lift your other arm and stretch it across the opposite side of your body, still keeping your arch in place.
A flat foot is a term used to described a collapsed arch. Medically, the term is pes planovalgus (for foot flatten and pushed outwards). There are varying degrees of ?flatness?. Though not all flat feet are problematic, however, when there are painful flat feet can cause significant discomfort and activity limitations. There are two kinds of flat feet - flexible (mobile) or rigid (stiff). A flexible flat foot is one where the foot retains motion, and the arch is able to be recreated when there is no weight on the foot. In contrast, a rigid flat foot is ?stuck? in the flat position regardless of whether or not there is pressure placed on the foot.
Causes
There are a variety of causes of flat feet. Flat feet can be genetic, acquired and develop over time. Young children and teens can have no arches. Injury can lead to flat feet. Tendon problems, and arthritis can lead to flat feet. Rigid flat feet may occur from a condition called tarsal coalition, where the bones in the back of the foot are genetically fused or locked together.
Symptoms
Repetitive exertive activity arch pain is usually sharp, and localized to a specific area, rather than the entire arch. Usually the pain occurs in the area just in front of the heel. It is present when first standing on the foot in the morning, but may decrease once you start walking around, but will, gradually becomes worse with continued walking or running. Swelling may be present. The pain subsides with rest, but stretching the arch while resting may cause the pain to return. Injury pain is constantly present, but worse when standing on the foot. This pain is localized to a specific area, but may radiate out from this area to the entire foot. The pain is sharp, and usually accompanied by swelling and occasionally "black and blue" discolorations. The pain due to the natural aging process is usually dull and aching, or stiff, and can be felt throughout the entire arch area, rather then in just one spot. This pain is present whenever weight bearing, and usually becomes worse with continued walking. The pain gradually subsides when resting, and usually does not return with stretching. Biomechanical defect pain is usually localized to a section of the arch, such as the inner, middle, outer, front, or back of the arch. This pain may be sharp or dull, but is always worse with continued walking.
Diagnosis
The doctor will take a brief history to determine how the injury occurred. If necessary, a thorough physical exam may be conducted to evaluate for any other injuries. Taking your workout shoes to the exam may also provide valuable information to the medical practitioner. Both feet will be physically and visually examined by the medical practitioner. The foot and arch will be touched and manipulated possibly with a lot of pressure and inspected to identify obvious deformities, tender spots, or any differences in the bones of the foot and arch.
Non Surgical Treatment
A new ankle foot orthosis known as the Richie Brace, offered by PAL Health Systems, has proven to show significant success in treating Stage II posterior tibial dysfunction and the adult acquired flatfoot. This is a sport-style brace connected to a custom corrected foot orthotic device that fits well into most forms of lace-up footwear, including athletic shoes. The brace is light weight and far more cosmetically appealing than the traditional ankle foot orthosis previously prescribed.
Surgical Treatment
The procedure involves cutting and shifting the bone, and then performing a tendon transfer. First, the surgeon performs a calcaneal osteotomy, cutting the heel bone and shifting it into the correct position. Second, the surgeon transfers the tendon. Reroute the flexor digitorum to replace the troublesome posterior tibial tendon. Finally, the surgeon typically performs one or more fine-tuning procedures that address the patient?s specific foot deformity. Often, the surgeon will lengthen the Achilles tendon because it is common for the mispositioned foot to cause the Achilles to tighten. Occasionally, to increase the arch, the surgeon performs another osteotomy of one of the bones of the midfoot. Occasionally, to point the foot in a straightforward direction, the surgeon performs another osteotomy of the outside portion of the calcaneus.
Prevention
Early in the treatment of arch pain, consideration needs to be given to the cause and strategies put in place to prevent it happening again. Advice should be sought on the adequacy of footwear. Stretching exercises should be continued long after the symptoms are gone. Foot orthoses should be used if structural imbalances are present. Activity levels and types of activities (occupational and sporting) need to be considered and modified accordingly.
Stretching Exercises
Easy Beginner Version. Start with your bare foot on a flat surface, toes spread out. Place a penny under the ball of your foot and the end of a pen under the middle of your arch (sticking out from the inside of your foot). Activate your arch by flexing your arch muscle. You should feel the muscles on the ball of your foot pushing down on the penny, but your arch shouldn't be pushing down on the pen. These tools help you (1) avoid rolling your foot and (2) avoid pressing down with your toes (as an extra tip, you can slide a business card under your toes before doing the exercise-when you activate your arch, you should be able to slide the business card out easily with your fingers). Do your best to keep your toes relaxed. Advanced Version. Once you're ready to move on, you can try this advanced version. It builds on the above exercise to incorporate full body twisting and balance, helping you to maintain proper arches while you move. Using the same ideas from above, stand on a flat surface in your bare feet with a penny under the ball of your foot and the end of a pen under your arch. This time, stand with your back a few inches away form a wall or a door. Lift your other leg (the one without the penny or pen) and stand on one foot. Use the wall for balance, if necessary. Lift one arm and stretch it across your body until you touch the wall or door on the opposite side, maintaining a straight back. Keep your foot straight and your arch on the penny but above the pen. Your arch will want to follow the movement and roll off, but you will need to activate it to stay stable during the movement. Lift your other arm and stretch it across the opposite side of your body, still keeping your arch in place.